
Scaphoid fractures
Understanding scaphoid fractures
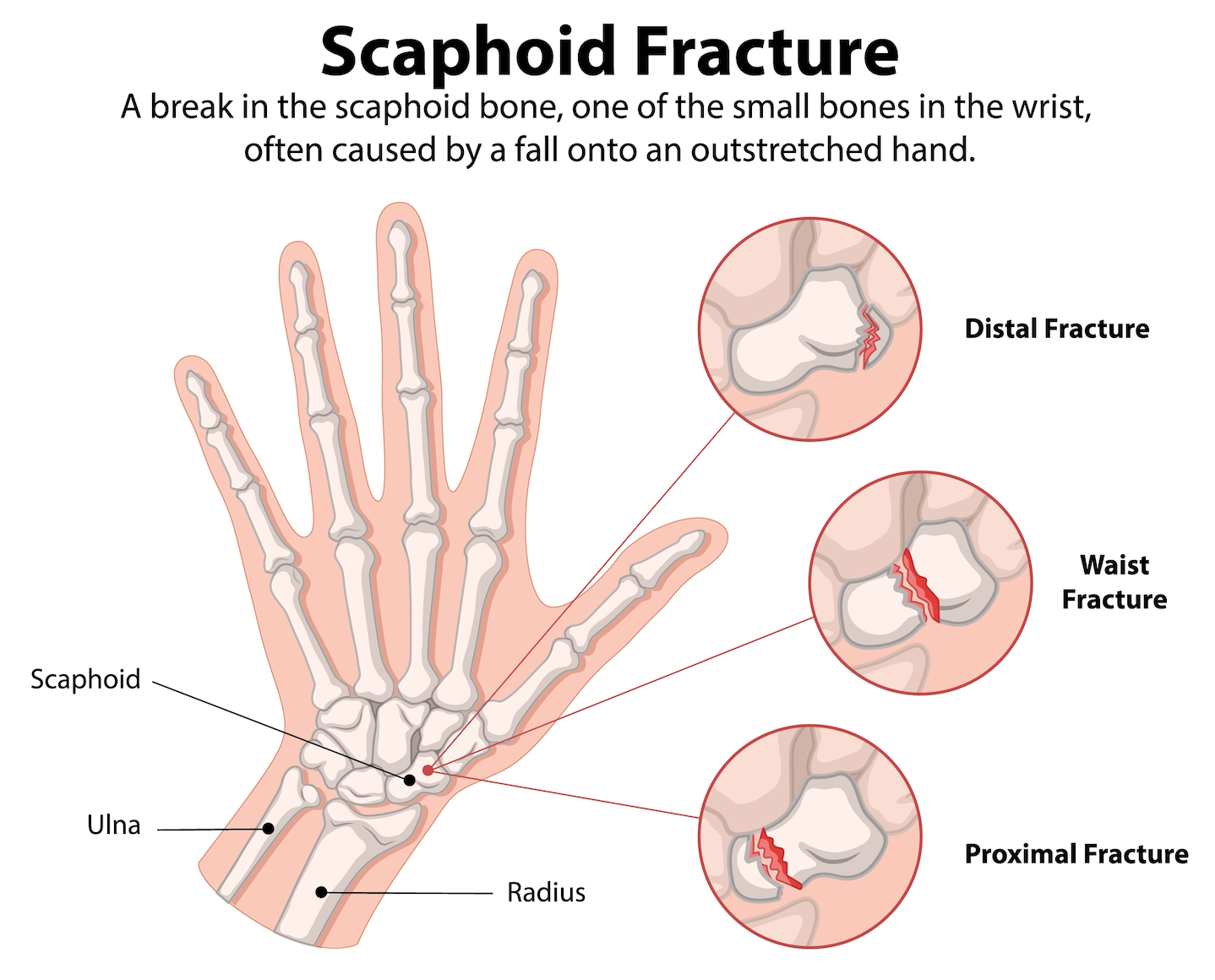
The scaphoid is a small kidney bean-shaped bone on the thumb side of your wrist. Fractures (breaks) typically occur from falls onto an outstretched hand. Men are affected twice as often as women.
The scaphoid's unique anatomy makes it vulnerable to healing problems. More than 75% of its surface is covered in cartilage, and it has a limited blood supply that enters through a small area on its back surface. This blood supply reaches the bone in a retrograde (backward) direction, meaning fractures closer to the thumb end heal more reliably than those near the forearm end.
Fractures occur most commonly at the bone's waist (middle section, 65% of cases), but can also affect the proximal pole (toward the forearm, 25%) or distal pole (toward the thumb, 10%).
-
Typical symptoms include:
Pain and swelling
Bruising
Reduced ability to move your fingers or thumb
Visible deformity of the digits
Numbness or tingling sensations
A wound (in open fractures)
-
X-rays: multiple specialised views are taken, including specific scaphoid views with your wrist positioned in extension and ulnar deviation.
CT scan: provides detailed images showing fracture pattern, displacement, and any deformity (humpback angulation). Modern cone-beam CT uses very low radiation doses. CT is useful to determine if surgery is required or if the fracture can be treated in a cast.
MRI: the most sensitive test for detecting fractures not visible on x-rays and can assess blood supply to the bone.
-
Treatment depends on several factors: fracture location, displacement, stability, and your individual circumstances.
Non-operative treatment
Stable, non-displaced fractures can be treated with cast immobilisation. Based on recent research (the SWIFFT study), many non-displaced fractures heal well with 6 weeks of casting, though some require longer immobilisation (8 weeks or more) until x-rays or a CT scan confirms healing.
Success rates are excellent for appropriately selected fractures: non-displaced fractures have approximately 90% union rates with casting. However, delayed treatment (more than 4 weeks) significantly increases the risk of nonunion.
You'll need to keep the cast clean and dry, and attend regular follow-up appointments to monitor healing.
Surgical fixation
Surgery may be recommended for:
Displaced fractures (2mm or more of separation)
Fractures with significant angulation or deformity
Proximal pole fractures
Fractures associated with other wrist injuries
Patients wanting faster return to work or sport
Non-displaced fractures where you prefer potentially faster healing
The procedure involves inserting a headless compression screw across the fracture to hold it in stable position while it heals. This can sometimes be done percutaneously (through tiny incisions without opening the fracture) or through open surgery, depending on the fracture pattern.
Surgery achieves 90-95% union rates. Following surgery, you'll typically wear a protective splint or cast for approximately 8 weeks.
Choosing between casting and surgery:
For non-displaced fractures, both options are reasonable. The SWIFFT study showed that while surgery may reduce nonunion rates slightly, it carries a 14% risk of potentially serious complications. I'll discuss both options with you, considering your occupation, activity level, and preferences to help you make an informed decision.
-
Nonunion means the fracture hasn't healed, typically diagnosed when a fracture fails to unite by 3 - 6 months after injury or surgery.
Risk factors for nonunion:
Delayed treatment (risk increases from 3% if treated within 4 weeks to 40% if treated after 4 weeks)
Proximal pole fractures
Displacement 2mm or more
Smoking
Advancing age
Why nonunion matters
Untreated scaphoid nonunion can lead to progressive wrist arthritis (SNAC - scaphoid non-union advanced collapse). The abnormal mechanics place excessive stress on the wrist joint surfaces, causing cartilage damage over time.
Treatment of nonunion
Extended casting: if the initial treatment was inadequate (insufficient immobilisation), extended casting with or without bone stimulation devices may achieve union, particularly within the first 6 months. Pulsed electromagnetic stimulation (such as the EXOGEN device) can be used alongside casting. Studies show approximately 69% achieve union by 3 months with this combination treatment.
Surgical treatment: most nonunions require surgery, which typically involves:
Cleaning out scar tissue from the fracture site to bleeding bone
Adding bone graft to fill any gaps and provide cells to stimulate healing
Stable fixation with screws, wires, or occasionally plates
Correcting any deformity (humpback angulation)
Bone graft options:
Non-vascularized bone graft: bone harvested from your pelvis (iliac crest) or forearm (distal radius), placed into the fracture site. Union rates approach 92%.
Vascularized bone graft: for nonunions with poor blood supply (avascular necrosis), bone with its own blood vessels can be transferred from your forearm or, in complex cases, from your knee using microsurgical techniques. This provides both structural support and improved blood supply.
Arthroscopic bone grafting: a minimally invasive technique where I use keyhole surgery to debride the nonunion site and pack in bone graft, fixed with wires. This approach has excellent union rates while preserving the wrist's blood supply. The wires endings are buried under the skin, and the wires are typically removed around 6 - 8 weeks later with a smaller surgical procedure. Wrist mobilisation commences upon removal of the wires.
If early arthritis is present (SNAC stage 1), I may combine nonunion surgery with radial styloidectomy (removing a small portion of bone where arthritis has developed).
-
Acute fractures:
Bone union typically takes 8 weeks or more for distal and waist fractures, and up to 16 weeks for proximal pole fractures. Following cast or splint removal, hand therapy helps restore wrist strength and motion. Full recovery may take 3 - 4 months.
Nonunion surgery:
Recovery is longer, typically requiring protected immobilisation for 8 - 12 weeks followed by progressive rehabilitation. The bone graft needs time to incorporate and remodel. You may not see final healing on CT or x-rays for 6 months or more.
-
Nonunion: as discussed above
Avascular necrosis: loss of blood supply to part of the bone, particularly the proximal pole (33% risk for proximal third fractures, 100% for the most proximal fifth)
Malunion: healing in an abnormal position
SNAC wrist: progressive arthritis from nonunion or malunion. There are various non-operative and operative ways to treat a SNAC wrist depending on the stage of arthritis. Treatment options include activity modification and pain management, limited wrist fusions (scaphoidectomy and four-corner fusion), proximal row carpectomy or total wrist fusion. I can discuss which option may be most appropriate for your individual situation.
Hardware complications: screws and wires can occasionally penetrate the joint surface or cause irritation
Scaphoid fractures require accurate diagnosis and appropriate treatment to prevent long-term complications. If you've injured your wrist and have pain in the anatomical snuffbox area, please seek prompt evaluation - early diagnosis and treatment significantly improve outcomes.