
Distal radius fractures
Understanding distal radius fractures
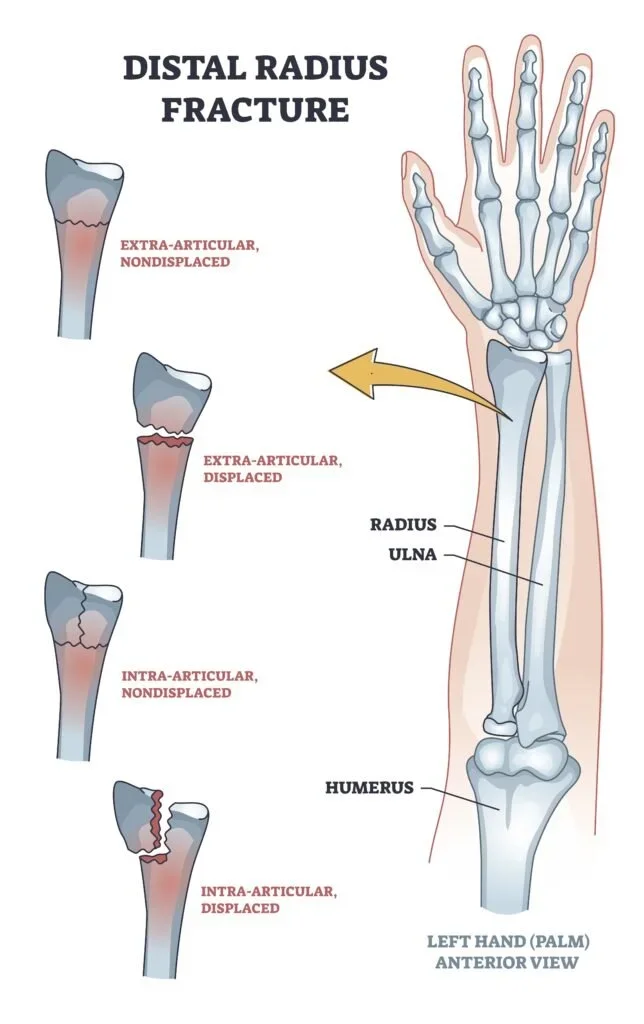
A distal radius fracture is a break in the larger forearm bone (radius) near the wrist. This is one of the most common fractures in adults, typically occurring from falls onto an outstretched hand. The fracture can range from a simple crack to complex breaks involving the joint surface and multiple fragments.
The distal radius has three functional columns that work together to support your wrist and hand:
Radial column: supports the thumb side of your wrist and helps maintain proper wrist alignment
Intermediate column: the main load-bearing area transmitting forces from your hand to your forearm
Ulnar column: supports the small finger side of your wrist
When these structures are disrupted by fracture, proper healing with good alignment is essential for maintaining wrist function.
-
Common symptoms include:
Immediate pain following a fall or injury
Significant swelling around the wrist and forearm
Visible deformity or abnormal wrist position
Bruising that may extend into the hand and fingers
Difficulty or inability to move the wrist
Numbness or tingling in the fingers (suggesting possible nerve involvement)
-
X-rays: multiple views assess the fracture pattern, displacement, and joint involvement.
CT scanning: provides detailed three-dimensional images showing the exact fracture configuration, particularly helpful for complex fractures involving the joint surface. CT scans are often obtained after initial reduction to guide treatment planning.
Assessment of associated injuries: distal radius fractures can occur alongside injuries to the wrist ligaments (particularly the scapholunate and lunotriquetral ligaments), triangular fibrocartilage complex (TFCC), and the ulnar styloid. These associated injuries may require specific treatment.
-
Treatment depends on fracture pattern, displacement, your age, activity level, and overall health.
Non-operative treatment
Stable, minimally displaced fractures can be treated with casting. The wrist is typically immobilised for 6 weeks with regular x-rays (usually weekly for the first 2 weeks) to ensure the fracture maintains acceptable position during healing.
Important: even with casting, some fractures shift position during the healing process. This is why close monitoring is essential.
Surgical fixation
Surgery is recommended when:
The fracture is significantly displaced or unstable
The joint surface is disrupted
The fracture cannot be held in acceptable position with casting alone
Multiple fragments require stabilisation
There are associated injuries requiring surgical treatment
The goals of surgery are to restore normal wrist anatomy, achieve stable fixation allowing early movement, and minimise the risk of complications.
-
Volar (palm-side) plating
The most common approach uses a plate applied to the palm side of the radius. This technique:
Provides stable fixation for most fracture patterns
Allows visualisation and reduction of the joint surface
Permits early wrist mobilisation
Positions the plate below the "watershed line" to minimise tendon irritation
The plate is secured with locking screws that engage the bone beneath the joint surface. Fluoroscopy (real-time x-ray) is used during surgery to ensure screws don't penetrate the joint or protrude dorsally where they could irritate tendons.
Dorsal (back-side) approach
Sometimes required for fractures with large fragments on the back of the wrist (dorsal ulnar corner fragments) or depressed joint surface fragments. During this approach, the extensor pollicis longus tendon (which extends your thumb) is typically repositioned away from the plate to prevent irritation or rupture.
Fragment-specific fixation
Some fractures require small specialised plates, screws, or pins to hold specific fragments.
Percutaneous pinning
Some fractures can be stabilised with pins (K-wires) inserted through small incisions. A technique using transverse K-wires can convert a complex multi-fragment fracture into a simpler pattern by holding the joint surface fragments together, making reduction easier.
External fixation and bridge plating
For severe, highly comminuted (shattered) fractures, contaminated open fractures, or patients with multiple injuries, an external fixator or bridge plate may be used. These devices span the fracture zone, maintaining length and alignment while allowing bone healing. Bridge plates are typically removed at 3-4 months.
Wrist arthroscopy
In selected cases, I may use wrist arthroscopy (a small camera inserted into the joint) during fracture surgery.
Arthroscopy allows me to:
Directly visualise the joint surface reduction
Identify and address cartilage damage
Diagnose associated ligament injuries (scapholunate, lunotriquetral, TFCC)
Guide precise placement of screws or pins
Treat significant soft tissue injuries when indicated
-
TFCC tears: up to 59% of distal radius fractures have associated TFCC injuries. However, TFCC tears are also common in older patients without symptoms. I only repair TFCC tears that cause demonstrable wrist instability during surgery.
Ulnar styloid fractures: these small bone fragments on the ulnar (little finger) side often occur with radius fractures. Most are stable after radius fixation. I assess stability after fixing the radius and only fix ulnar styloid fractures if they cause ongoing wrist instability or if the fracture is displaced more than 2mm at the base.
Distal ulna fractures: when the smaller forearm bone (ulna) is also broken, displaced fractures typically require separate fixation to allow early movement and reduce nonunion risk.
-
Early phase (0-2 weeks post-surgery):
Elevation is crucial to minimise swelling and pain. Keep your hand elevated above your heart as much as possible. I'll see you around 2 weeks post-operatively to check your wound and assess early healing. At this appointment, I'll also clinically assess your extensor pollicis longus tendon function - this tendon can occasionally rupture after distal radius fractures even with successful treatment.
Intermediate phase (2-6 weeks):
Gentle finger and wrist exercises begin, often with hand therapy guidance. The exercises help prevent stiffness while protecting the healing fracture. If temporary k-wires were used, these are typically removed around 6 weeks.
Later phase (6-12 weeks):
Progressive strengthening exercises and increasing activity. Most patients regain functional wrist movement by 3 months, though full recovery can take 6-12 months, particularly for complex fractures.
-
Stiffness: the most common complication. Hand therapy plays a crucial role in preventing and treating stiffness. Early appropriate movement is essential.
Malunion: if the fracture heals in poor position (either from inadequate initial treatment or loss of reduction), this can cause pain, limited movement, wrist instability, or ulnar-sided wrist pain from abnormal loading. Malunion may require corrective surgery (osteotomy) to realign the bone.
Hardware irritation: plates and screws can occasionally irritate tendons, particularly the flexor or extensor tendons. If this occurs, hardware removal may be necessary once the fracture has healed (typically after 12-18 months).
Nerve problems: carpal tunnel syndrome can develop or worsen after distal radius fractures. Temporary numbness from nerve swelling usually resolves, but persistent symptoms may require carpal tunnel release.
Complex regional pain syndrome (CRPS): an uncommon but significant complication causing disproportionate pain, swelling, and stiffness. Early recognition and intensive hand therapy are essential for managing CRPS.
Tendon rupture: extensor pollicis longus rupture can occur weeks to months after fracture (even with successful treatment) due to disrupted blood supply and attrition. This requires tendon transfer surgery for restoration of thumb extension.
Arthritis: fractures involving the joint surface carry increased risk of developing wrist arthritis over time, even with anatomical reduction.
-
If a distal radius fracture has healed in poor alignment (malunion), this can cause:
Chronic wrist pain from abnormal loading
Limited wrist movement (particularly rotation and flexion/extension)
Wrist instability
Ulnar-sided wrist pain
Surgical correction involves cutting the bone (osteotomy), realigning it to restore normal anatomy, and securing it with a plate and bone graft. For simple malunions, this can be done freehand. Complex three-dimensional deformities may benefit from computer-guided planning and correction.
The maximum acute correction that soft tissues typically tolerate is approximately 10mm. Larger corrections may require combining radius correction with ulnar shortening (if ulnar-sided symptoms are present).
Distal radius fractures require accurate diagnosis and appropriate treatment to restore wrist function and prevent long-term complications. If you've sustained a wrist fracture, prompt evaluation ensures the best possible outcome.