
Cubital tunnel syndrome
Understanding the condition
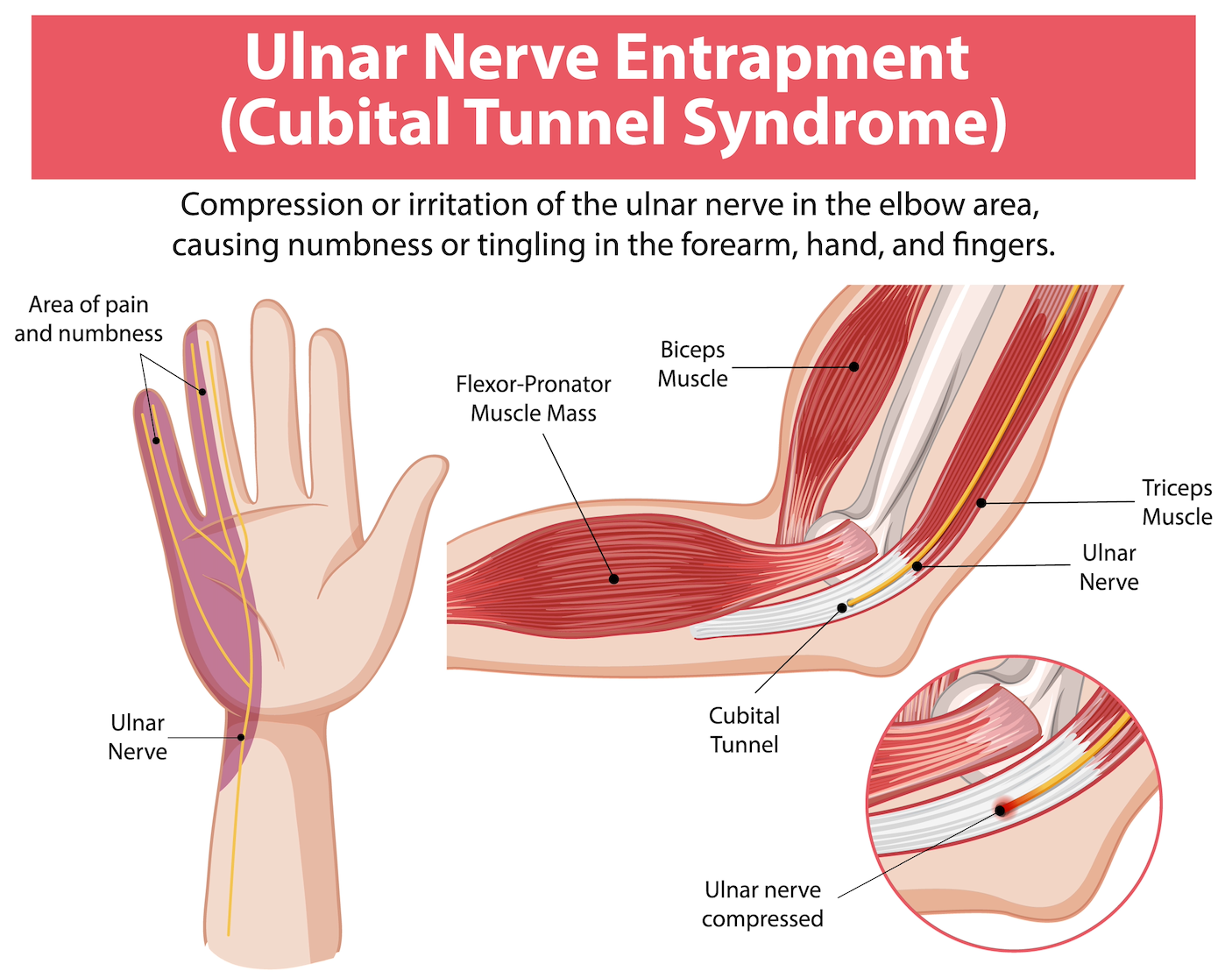
Cubital tunnel syndrome results from pressure on the ulnar nerve as it passes through a confined space at the elbow's inner aspect - the area known as the "funny bone." This nerve supplies sensation to your little finger and half of your ring finger, while also powering the small intrinsic muscles that control fine hand movements.
Why it develops
Many cases emerge spontaneously without identifiable triggers. However, the tunnel's diameter can become reduced by elbow joint arthritis or remote trauma affecting the bone architecture.
-
Early presentation:
Altered sensation or tingling affecting your little and ring fingers typically appears first. These symptoms often fluctuate initially but may eventually become persistent. Common provocative positions include:
Prolonged elbow flexion (phone conversations, reading in bed)
Pressure on the inner elbow (leaning on armrests or desks)
Sleeping with the elbow habitually bent
Progressive symptoms:
As compression worsens, numbness becomes continuous and hand weakness develops. Advanced cases show visible muscle atrophy - particularly noticeable in the web space between thumb and index finger on the hand's dorsal surface - accompanied by deteriorating grip strength and fine motor control.
Diagnostic evaluation may include elbow radiographs and electrodiagnostic nerve studies to confirm the diagnosis and assess severity.
-
Activity modifications often provide relief in early-stage disease:
Ergonomic adjustments (using telephone headsets to avoid prolonged elbow flexion)
Avoiding direct pressure on the elbow's medial aspect or using protective padding
Night time positioning aids - a towel wrapped around the elbow or therapist-fabricated splint limiting flexion during sleep
These strategies can be curative when implemented early in the disease course.
-
Surgery becomes necessary for advanced cases or when conservative treatment fails. The primary objective is preventing progressive motor deterioration and muscle wasting characteristic of severe untreated compression. While surgery frequently improves sensory symptoms, halting motor decline represents the critical goal.
A cubital tunnel release involving opening the tunnel's constraining roof to create additional space and decompress the nerve. In some cases, the following procedures may also be required:
Nerve transposition: relocating the nerve anteriorly away from the cubital tunnel
Medial epicondylectomy: removing a portion of the tunnel's bony floor to expand its volume
I'll recommend the approach best suited to your specific pathology and symptom pattern.
-
Results correlate directly with pre-operative compression severity. Sensory recovery often occurs but may progress gradually over many months. Surgery typically arrests motor progression, though strength improvements tend to be slow and incomplete.
Mild cases generally achieve complete symptom resolution. More severe presentations carry less predictable outcomes regarding full neurological recovery. I'll talk you through expected results and timelines based on your examination findings and diagnostic studies, and your therapist will guide your rehabilitation.
Persistent numbness or hand weakness warrants evaluation. Contact your general practitioner if you're experiencing these symptoms.