
Boutonnière deformity
Understanding the condition
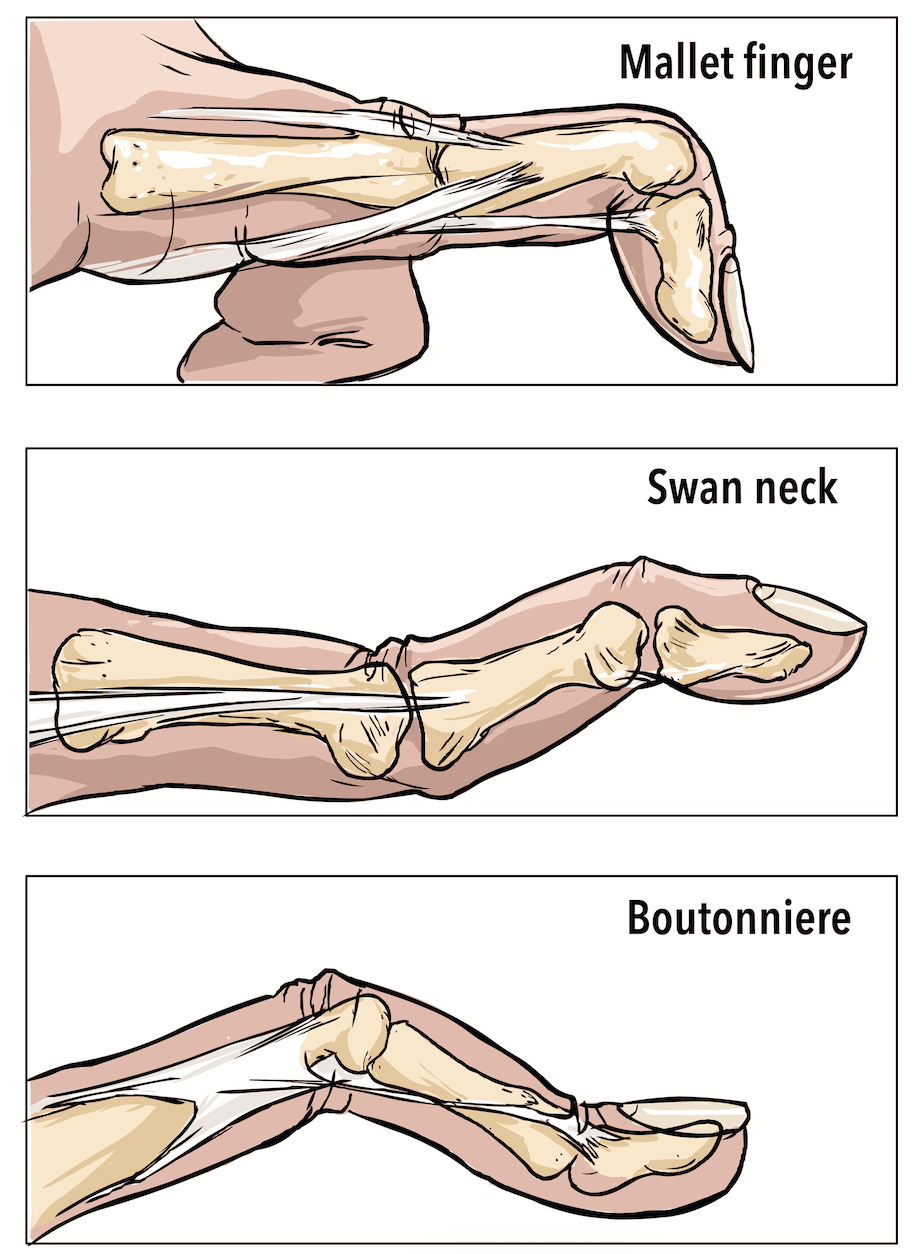
Boutonnière deformity describes a characteristic finger posture: flexion at the proximal interphalangeal (PIP) joint combined with hyperextension at the distal interphalangeal (DIP) joint. While traumatic injury (typically jamming or stubbing mechanisms) represents the most common cause, this deformity can also develop secondary to arthritic conditions.
The mechanism of injury
In normal finger mechanics, extensor forces balance between the central slip (inserting at the middle phalanx base) and the terminal tendon (inserting at the distal phalanx). When trauma or a laceration disrupts the central slip, it loses its ability to extend the PIP joint, which subsequently drops into flexion. The extensor mechanism then redirects entirely through the terminal tendon, creating excessive DIP joint extension and limiting terminal joint flexion.
-
Pain and swelling localised to the PIP joint (middle knuckle)
Finger rests in flexion at the PIP joint
Inability to actively extend the PIP joint
Reduced DIP joint flexion (cannot fully curl the fingertip toward palm)
Diagnosis can be challenging initially, as the characteristic posture may not manifest for days or weeks post-injury. Early presentation often resembles common PIP joint sprains with pain, oedema and stiffness.
Radiographs evaluate for fractures and confirm joint alignment. Ultrasound imaging is occasionally helpful for diagnostic confirmation.
-
Lacerations
Open injuries allow direct tendon repair through surgical intervention.
Closed injuries
Jamming injuries typically respond to splinting protocols. The splint maintains PIP joint extension while permitting DIP joint motion. Various splint configurations exist depending on your finger anatomy.
Splinting duration ranges from four to eight weeks. A hand therapist typically monitors your progress, as proper splint compliance is crucial for optimal tendon healing.
-
Most splint-treated injuries heal with satisfactory functional outcomes, though achieving maximum recovery may require several months. Some patients experience residual limitations - incomplete PIP extension and/or restricted DIP flexion.
Treatment failure
Occasionally, central slip healing proves inadequate. Extended immobilisation may be attempted. If conservative management fails, surgical reconstruction options exist, which I can discuss with you if necessary.
Boutonnière deformity requires proper diagnosis and treatment for optimal outcomes. If you've injured your finger and notice difficulty straightening the middle joint, please seek evaluation - early recognition and appropriate splinting improve prognosis.